
If you work in oncology or infusion, you already know that biosimilars aren't coming; they're here. For most drugs, your team has figured out the clinical piece. You know the science, you understand interchangeability, and you've read the FDA approvals.
The part that keeps tripping people up isn't clinical. It's communication.
 Here's what that looks like on the unit: A nurse gets an order for a biologic. There are four biosimilars approved for that drug, two of them on your formulary, but which one does your health system prefer for inpatient use? What about outpatient? Does the answer change depending on which payer the patient has? And if a biosimilar received FDA approval last month, has your team addressed it yet, or is that nurse about to send a message to pharmacy asking a question that five other nurses already asked this week?
Here's what that looks like on the unit: A nurse gets an order for a biologic. There are four biosimilars approved for that drug, two of them on your formulary, but which one does your health system prefer for inpatient use? What about outpatient? Does the answer change depending on which payer the patient has? And if a biosimilar received FDA approval last month, has your team addressed it yet, or is that nurse about to send a message to pharmacy asking a question that five other nurses already asked this week?
So why is getting the right information to the right person so hard?
The challenge with biosimilars is that the information your team needs isn't static. Preferred agents change when contracts are renegotiated, and payers make their own coverage decisions, which means the preferred inpatient biosimilar and the preferred outpatient biosimilar for the same drug can be completely different, and both can shift year to year. Meanwhile, the pipeline keeps moving. Take denosumab: the number of approved biosimilars for that drug alone has grown significantly in a short period, and more are on the way.
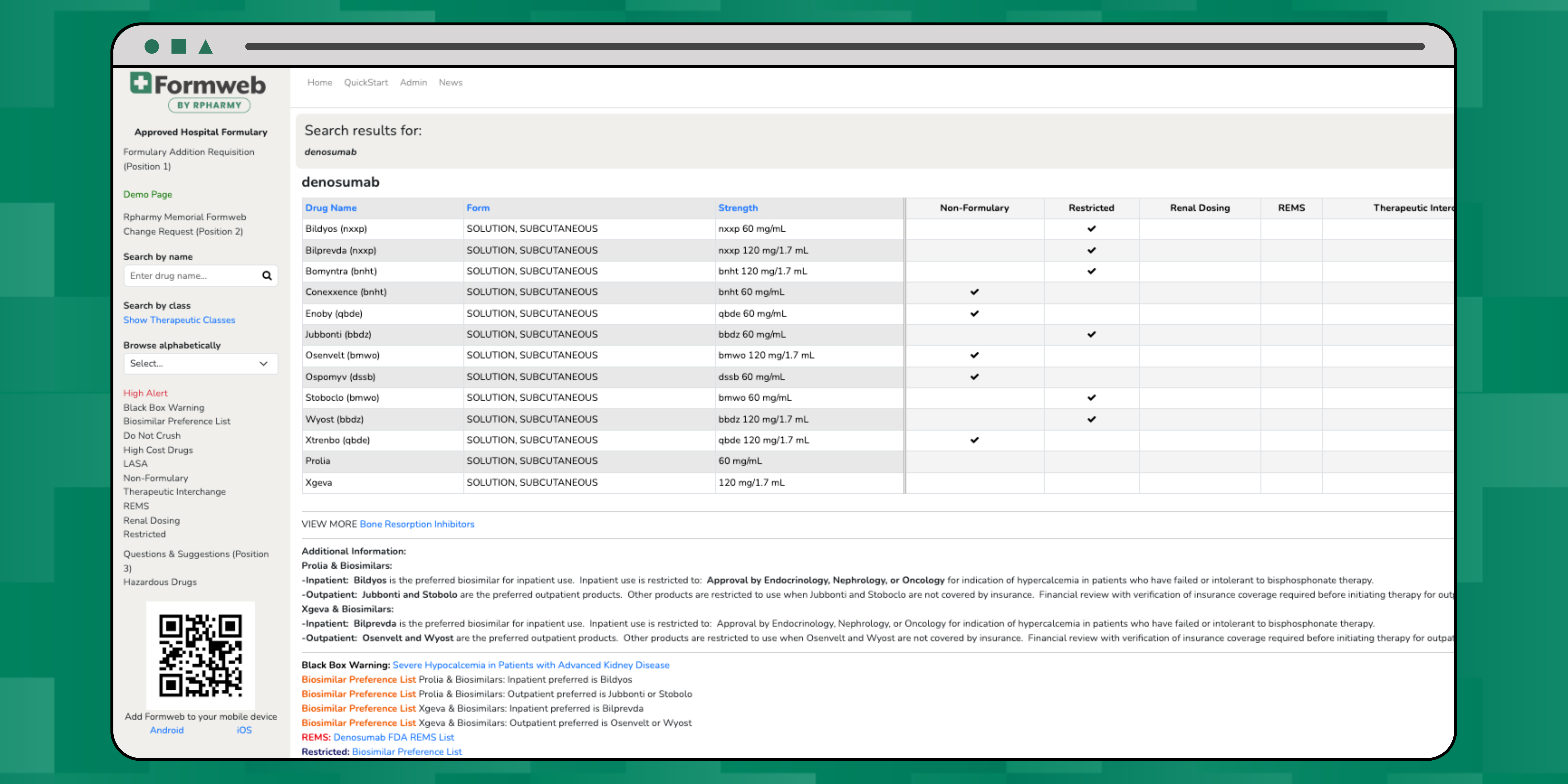
In Formweb, approved and preferred biosimilars are easily documented and communicated as can be seen here with the denosumab listing on the demo site.
Most health systems are trying to manage this through emails, shared drives, and verbal updates at huddles, and that approach works until it doesn't. Until a nurse administers the non-preferred agent because she didn't know the preference had changed. Until a physician orders a biosimilar that requires pre-approval, no one catches it until after dispensing. Until a patient's insurer denies a claim because the health system used a biosimilar, the payer doesn't cover for outpatient use.
 What we're seeing from health systems that are managing this well is that they've stopped treating biosimilar communication as a one-time announcement and started treating it as a living part of their formulary. That means making the preferred agent visible at the point of care, not buried in a PDF on the intranet or in last quarter's P&T update, but right there when a clinician is making the decision. It means being explicit about the inpatient-versus-outpatient distinction, because those differences can't be assumed. It means having a plan for when a new biosimilar enters the market, so the answer to "what do we do with this one?" is ready before the questions start coming in.
What we're seeing from health systems that are managing this well is that they've stopped treating biosimilar communication as a one-time announcement and started treating it as a living part of their formulary. That means making the preferred agent visible at the point of care, not buried in a PDF on the intranet or in last quarter's P&T update, but right there when a clinician is making the decision. It means being explicit about the inpatient-versus-outpatient distinction, because those differences can't be assumed. It means having a plan for when a new biosimilar enters the market, so the answer to "what do we do with this one?" is ready before the questions start coming in.
What does this mean for oncology nurses and nurse educators on the front line?
Biosimilar education is still catching up to biosimilar availability. Patients ask questions, physicians ask questions, and increasingly, the nurse is the one in the room when those questions come up. Having clear, accessible information about what your health system has decided and why isn't just operationally useful. It's part of delivering confident, informed care.
Biosimilars are one of the more meaningful opportunities health systems have right now to manage drug costs without compromising clinical outcomes, but that opportunity only translates into savings if the communication infrastructure keeps pace with the clinical one. The science is there. The question is whether the information is where it needs to be, when it needs to be there.
Want to see how other health systems are actually doing this? We recently hosted a short webinar on exactly that: how our clients document and communicate biosimilar information in real time. It's 15 minutes and worth every one of them. Watch it here.

